

Acute Peroneal Tendon Subluxation
Summary
Acute peroneal tendon subluxation involves the displacement of one or both peroneal tendons over the bone (fibula) on the outside of the ankle following an acute injury. These tendons are held in place by a strong fibrous tissue called the superior peroneal retinaculum which tears, stretches, or avulses off a fragment of fibula bone during the injury. This injury to the superficial peroneal retinaculum creates space for the peroneal tendon to pop over (sublux) the fibula. Acute peroneal subluxations occur following a sudden injury to the ankle and lead to considerable pain. Non-surgical treatment of immobilization to allow healing can be tried, but many patients require or will benefit from a surgical repair to quicken their recovery and minimize their chance of developing chronic peroneal tendon subluxation.
Anatomy of the Peroneal Tendons
The peroneal tendons are the main tendons that run along the outside part of the foot and ankle. There are two peroneal tendons (Figure 1). The first is called the peroneus brevis. The term “brevis” implies short. It is called this because it has a shorter muscle and starts lower in the leg. It then runs down around the back of the bone called the fibula on the outside of the leg and inserts (i.e. connects) to the fifth metatarsal. This is on the outside part of the foot. The peroneus longus takes its name because it has a longer course. It starts higher on the leg and runs all the way underneath the foot to insert or connect onto one of the bones (1st metatarsal) on the inside of the foot.

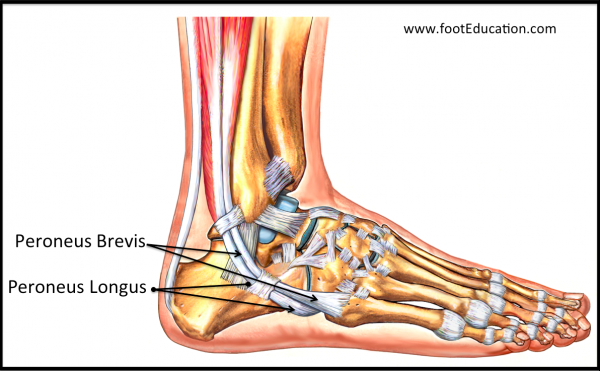
Figure 1: Tendons of the Peroneus Longus and Brevis
Both tendons, however, share the major job of turning the foot outwards (everting). The tendons are held in a groove behind the back of the fibula bone and have a roof made of ligament-like tissue called the superior peroneal retinaculum (SPR). The SPR is the main restraint to peroneal tendon subluxation. In peroneal tendon subluxation the SPR is injured, which can cause one or both of the peroneal tendons to be prominent and pop over the edge of the prominent fibula (subluxation).
Clinical Presentation
A patient with an acute peroneal tendon subluxation will experience pain on the back and outer part of their ankle following an injury. At the time of the injury, one of the two tendons that is normally positioned behind the fibula bone on the outside of the ankle, pops around the fibula. When this occurs, the tendon can damage both restraining structures, including the soft tissue, known as the “superior peroneal retinaculum” (SPR), and also occasionally the fibula bone itself. The pain following an acute peroneal tendon subluxation can be quite significant. This injury usually leads to a pronounced limp and, in some cases, an inability to walk.
Physical Examination
On exam, patients with an acute peroneal tendon subluxation will have quite marked tenderness on the back part of the distal fibula, which is the bone on the outside of the ankle. When the foot is forced in an outward direction (everted), one of the peroneal tendons may be noticable and even pop over the edge of the prominent fibula (subluxation). This maneuver in the acute setting will create a significant amount of discomfort.
Imaging Studies
X-rays of patients with an acute peroneal subluxation are often normal, but may show a small rim of bone that has been pulled off (avulsed) of the back part (posterior) of the fibula.
An MRI is usually not required to diagnose and treat an acute peroneal tendon subluxation. However, if an MRI is performed, it will typically demonstrate an injury to the thick fibrous tissue called the superior peroneal retinaculum (SPR), which normally holds the peroneal tendons in place behind the fibula. An MRI will also demonstrate any bony avulsion injuries associated with the displacement of the peroneal retinaculum and any associated damage to the peroneal tendons themselves.
Treatment
Treatment of an acute peroneal tendon subluxation can be non-surgical or surgical. Treatment requires that the tendons be kept back in position behind the fibula and that they be held there until the soft tissues and any bony fragment has healed. This requires a period of approximately six weeks of immobilization (cast or walking boot). Following that, a rehab program is gradually started to restore the strength and function of the peroneal tendons.
Nonsurgical treatment for acute injuries in active young athletes has a relatively high chance of the peroneal tendon subluxation recurring and becoming chronic. Therefore, in active patients, surgical repair and stabilization of the injured superior peroneal retinaculum (SPR) is often the treatment of choice, although in some instances a course of immobilization may be tried. In addition, surgical treatment of an acute peroneal subluxation is necessary when the peroneal tendons cannot be contained behind the bone (fibula) on the outside of the ankle either because the associated avulsed bone fragment is too large, or by the nature of the shape of the fibula.
Some patients who suffer an acute peroneal subluxation will go on to develop chronic peroneal subluxations. This is more likely in injuries that are missed. Patients with chronic peroneal tendon subluxation commonly require surgical treatment.
Edited October 12, 2023
Previously Edited by: Daniel Cuttica, DO, and Samuel Dellenbaugh, MD
sp/10.12.23