

Metatarsal Shaft Fractures
Edited by Marcus Coe, MD
Summary
The metatarsals are the long bones in the forefoot that lead up to the toes. Metatarsal shaft fractures are common injuries, and cause pain and swelling in the mid and forefoot. They are typically caused by a trauma, such as the drop of a heavy object on the foot, or the sudden bend of the forefoot (i.e. a trip and fall on uneven ground). Metatarsal shaft fractures can also be caused by direct loading and twisting of the foot, such as what might occur in an automobile accident. If bones are fragile (Osteoporosis), it takes minimal trauma to cause these types of fractures, such as a miss-step or a sudden twisting movement. In addition to acute fractures of the metatarsals, repetitive intense activity (i.e. military marching) or a change in intensity of a particular activity can lead to a “stress fracture” of one of the metatarsals. Most metatarsal shaft fractures can be treated non-surgically, with limited weight bearing in a stiff-soled shoe or a boot for 6 to 8 weeks, provided that the bones are in an acceptable position. Some displaced fractures will benefit from surgery to reposition and stabilize the bones.
Clinical Presentation
Metatarsals are the five long bones that connect the forefoot to the midfoot. A break (fracture) in one or more of the metatarsals is often associated with significant swelling, and also pain in the arch of the foot or at the pads of the forefoot. Usually the soft tissue overlying the bones remains intact, but in some instances, the bones will break through the skin, creating an open injury, which is a surgical emergency. Common mechanisms for having metatarsal shaft fracture(s) include falling from a high height and landing on the feet, jamming the foot into the brake pedals in the course of a motor vehicle collision, loading the foot and twisting it in the course of changing directions during a sporting event, and most commonly, dropping a heavy object on the forefoot. Overloading of the foot can also result in stress fractures of the metatarsal. This can occur when either: 1) the force on the foot is greater than the bone can handle, or, 2) everyday forces cause fracture because of poor bone quality.
Physical Exam
In the case of an isolated metatarsal shaft fracture, there will be tenderness and swelling localized to the injured area. In the case of multiple metatarsal fractures, the painful, swollen area will be larger and will correlate to the involved bones. During the acute phase of the injury, there may be bruising that extends toward the toes. There may also be some numbness in the toes. The purpose of the exam is to assess the position of the toes, the toe alignment, as well as the blood supply to the toes.
It is important to assess the position of the metatarsal heads. These are the ends of the metatarsals that represent the “ball of the foot”. This is the area that we walk on, and it is possible to have a problematic position of the metatarsal head, resulting from a displaced metatarsal fracture.
Imaging Studies
Plain x-rays of the foot will usually identify the fracture (Figure 1). The location and pattern of the fracture will be identified and assessed, along with the position of nearby bony architecture. The rotation and angulation at the fracture site are all things that the treating physician will need to consider. In the case of a metatarsal stress fracture, the original x-ray may be read as normal, so often a second x-ray is recommended when there is suspicion for a stress fracture. An additional x-ray 3-4 weeks post injury is helpful in identifying how healing is progressing in the affected bone.
Figure 1: Metatarsal Fractures on X-ray


Treatment
Most metatarsal fractures can be treated non-surgically. If the fractured metatarsals are in an acceptable position, they can be treated without surgery. In rare occasions, manipulation of the bone to reposition them in an acceptable position is necessary. Occasionally, an “open reduction internal fixation” procedure is required to stabilize the bone. This may involve placement of small plates and/or screws, or using pins to realign the bone. Multiple metatarsal fractures are rare and normally are treated with restricted weight bearing. Walking on an injured foot with multiple metatarsal fractures is not recommended, and may cause further displacement of the broken bones and ultimately cause the need for surgical intervention.
Treatment of a single metatarsal fracture involves protecting the injured foot until the bone is healed. During this time, limited weight bearing in a stiff soled boot or a very stiff soled shoe is recommended to support the fracture. It typically takes 6-8 weeks for the bone to heal and get strong enough for the patient to resume full weight bearing in a normal shoe. Despite being able to walk, patients with a metatarsal fracture are advised to avoid excessive walking, especially on uneven ground, to eliminate the risk of displacement. It is often 4 to 6 months before a full recovery is obtained (ex. return to unrestricted activities such as jumping and sprinting).
Smoking slows down the bone healing process, and normally fracture healing is slower in smokers. Smoking cessation is recommended to all patients with broken bones. Taking daily vitamin D and calcium is also recommended treatment your doctor may suggest.
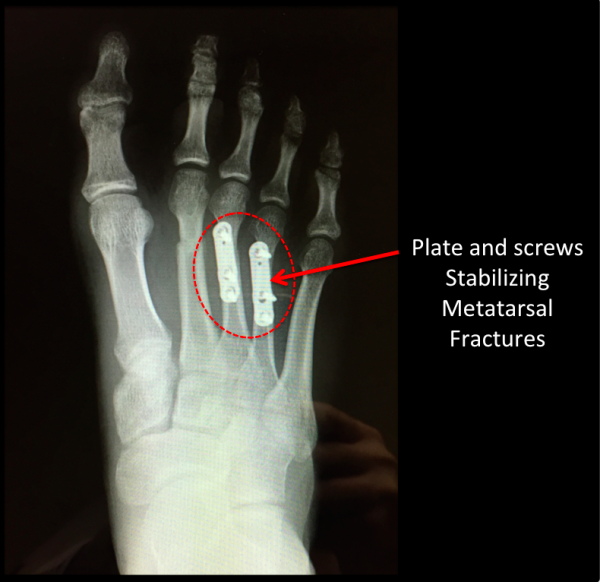
Surgery may be indicated in the case of either a significantly displaced metatarsal shaft fracture, or in the case of multiple displaced metatarsal shaft fractures (Figure 2). There is some suggestion that surgical stabilization for a displaced metatarsal shaft fracture can produce a slightly faster recovery time, albeit with the associated risks of surgery. These risks include infection and residual numbness around the toe or surgical site. In rare cases, excessive scar formation around the surgical site may cause toe deformity in the long term.
Figure 2: Surgical Stabilization of Metatarsal Fractures

Edited on August 22, 2017
(Previously edited by Gwyneth DeVries, MD FRCSC and Hossein Pakzad, MD)
mf/ 6.11.18