
Overload Heel Pain Syndrome
Edited by Sam Dellenbaugh, MD
Summary
Overload heel pain syndrome is an uncommon cause of heel pain, unlike plantar fasciitis which is by far the most common cause. However, there are some patients that have overload heel pain syndrome as the primary source of their heel pain. These individuals will have pain that is centrally located in the heel rather than towards the inside of the heel pad, such as is typical in plantar fasciitis. Individuals with certain foot patterns, such as high arched feet, relative weakness of the calf muscle, or dysfunction of the Achilles tendon, may be predisposed to overloading the heel with resulting symptoms. In addition, thin soft tissue padding (fat pad atrophy) over the heel may also lead to these symptoms. Diagnosis is usually based on patient history and clinical examination. Treatment is almost invariably non-operative and focuses on increasing the padding over this area, helping to disperse the forces away from the tissue, as well as avoiding aggravating activities, and weight loss if necessary.
Clinical Presentation
Patients with overload heel pain syndrome describe the feeling of pain directly at the base of their heel. The most common cause of heel pain is due to plantar fasciitis. However, overload heel pain syndrome can also be a source of significant heel pain. In overload heel pain syndrome, essentially the soft tissues and bone directly under the heel bone (calcaneus) are aggravated by direct repetitive pressure from standing and walking. Factors which predispose an individual to overload heel pain syndrome include:
- a prominent heel
- thin soft tissue overlying the bone of the heel
- certain foot shapes (ex. high arches)
- excessive weight.
Physical Examination
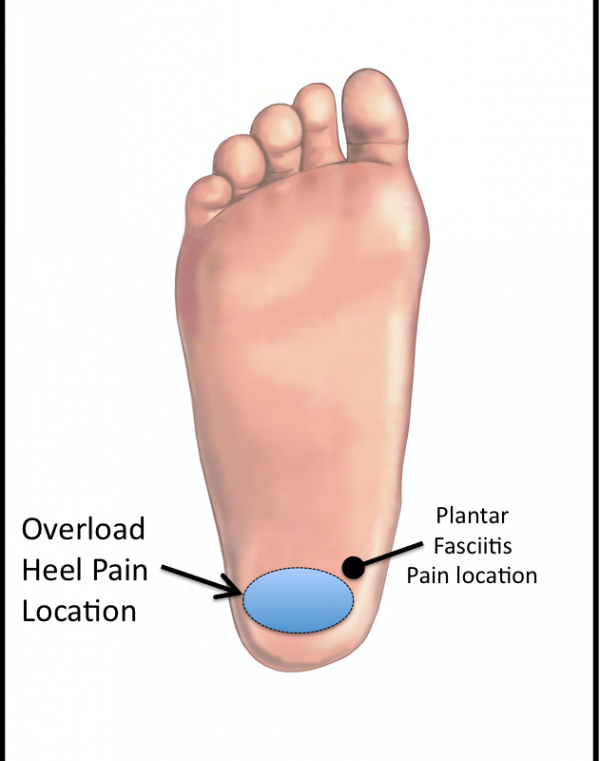
Physical examination will localize the tenderness centrally in the heel pad. This is more central than the pain that is characteristic of plantar fasciitis, which is slightly more to the inside but still in the heel area (Figure 1). Individuals with overload heel pain syndrome will often have increased ankle dorsiflexion (the ability to move the foot up towards the shin). This makes the heel more prominent. The area of pain is differentiated from pain related to interstitial Achilles tendonitis, retrocalcanceal bursitis and plantar fasciitis. Excessive weight may also be present.
Figure 1- Overload Heel Pain Syndrome -common location of pain
Imaging Study
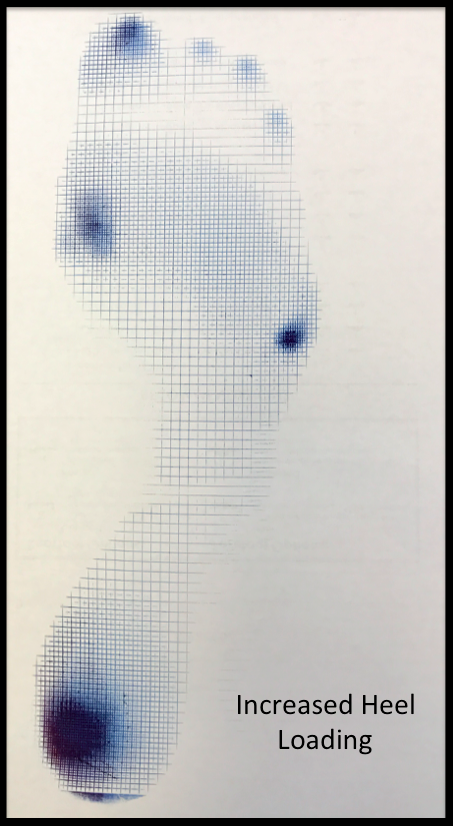
A Harris mat or other method of measuring the pressure that the foot absorbs while walking will often show an intense localized force concentrated on the heel area (Figure 2).
Figure 2: Harris Mat showing concentrated load over the heel region
Often plain x-rays are normal, although they may demonstrate an increased calcaneal pitch angle (the angle of which the lower part of the heel bone meets the floor). In some instances, there may be a small bone spur that points towards the floor. This is different than the characteristic bone spur that may be seen with plantar fasciitis, which points more toward the front of the foot. An MRI may reveal an increased area of edema, and possibly a bursa (fluid filled sac) over the prominent area of the heel. An MRI may also reveal less fatty tissue and soft tissue over the heel.
Treatment
Non-Operative Treatment
Treatment is usually non-operative. It involves allowing the heel area to be protected from increased repetitive loading, allowing the tissues in this area to heal. This can be done by limiting standing and walking. In marked cases, immobilization in a walker or cast may be beneficial for a short period of time. Because of atrophy of the fat pad, the use of a gel pad or other padding to absorb the shock and disperse the force over a wider area can also be beneficial.
Surgical Treatment
Surgical treatment is reserved for very unusual situations. If there is a prominent spike of bone that is a source of symptoms, this could be removed. However, this is unusual. In addition, if the foot pattern is markedly abnormal, such as might occur in a high arched foot or someone with an incompetent Achilles tendon, then a reconstructive surgery to address these issues may indirectly help the overload heel pain.
Edited on August 13, 2017
Previously Edited by Paul Juliano, MD
mf/ 6.4.18