
Claw Toes (also Hammer Toes)
Summary
Claw toes develop in many people as they age, and can make fitting into restrictive shoes uncomfortable. This condition can create symptoms in one, or all, of three places:
- On the top of the toes if they rub against the shoes (dorsal corn)
- On the tips of the toes if they jam into the soles of the shoes (painful toe tips)
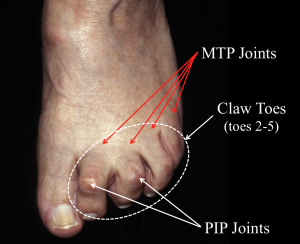
- At the base of the toes (metatarsophalangeal (MTP) joints) as the MTP joint may become unstable with repetitive loading.
In addition, claw toes are often associated with forefoot pain (metatarsalgia), as the MTP joints commonly become overloaded or even displaced in patients with pronounced claw toes. Subluxation is the upward displacement of the toe relative to the metatarsal head or “ball of the foot.” This leaves the metatarsal heads prominent and subject to excessive overload. Patients with this problem often describe their symptoms as “walking on marbles.”
Printable handout
Clinical Presentation
Claw toes result from an inherent muscle imbalance. It is common for patients to develop claw toes as they get older. It is particularly common if there is a family history of the condition. Patients develop claw toes when the long muscles originating from the lower leg overpower the smaller muscles in the foot. This imbalance leads to flexion at the proximal interphalangeal joint, and extension at the metatarsal phalangeal joint, creating the clawing effect. This condition can also occur following an injury (post-traumatic), if one of the tendons is injured, or if there is a compartment syndrome affecting the small muscles of the foot. Commonly, clawing of the toes develop if the calf muscles are tight. If the calf is tight, there is increased recruitment of the muscle that pulls the toes upward (the extensor digitorum longus) to assist in pulling the foot up to clear the ground while walking in preparation for the next step.
Claw toe deformities typically involve all four lesser toes (toes 2-5). It is not uncommon for the second toe to have the most pronounced deformity, but a close look at all four toes will often demonstrate that the deformity is present in each toe (See Figure 1). It is uncommon for the big toe to develop clawing, although this does happen in certain conditions, including Charcot Marie Tooth disease. The term ‘hammer toe’ is almost synonymous with claw toes. The main difference between these two conditions is the position of the distal interphalangeal joint (DIP joint). In hammer toes, this joint is extended and in a claw toe it is flexed. However, it can sometimes be difficult or impossible to clinically differentiate between “claw toes” and “hammer toes”.
Physical Examination
On physical examination, the physician will want to identify the main areas of the patient’s tenderness. This will give some indication as to the cause of the pain. If the tenderness is on the top of the toes and is associated with some callus formation, symptoms are likely from direct pressure on the top (dorsal aspect) of the toe. If tenderness occurs on the tip of the toe, this may be from the pressure of the tip of the toe (“hammering”) into the sole of the shoe. In addition, whether or not the toes are “flexible” or “fixed” is important. Each joint will be evaluated to assess whether this joint can return to its normal position. The overall alignment of the toes is important, as well as the sensation, motor function, and blood supply of the toes.
Conditions Associated with Claw Toes/Hammer Toes
Claw toes/Hammer toes – Dorsal Corn (026)
Claw toes/hammer toes are foot deformities that impact the proximal and distal interphalangeal joints (PIP and DIP) of the toes. A claw toe deformity impacts both joints, while a hammer toe deformity impacts the PIP. In both settings, a dorsal corn can develop on the top side of the abnormal bent joint (Figure 1 -PIP joints). A dorsal corn consists of thickened and hardened dead skin (callus) that forms as a result of friction from the bent joint rubbing against footwear. Patients will present with pain and a hardened prominence on the top of the abnormal joint. Treatment options for dorsal corns include wearing loose-fitting footwear and putting protective pads in footwear to prevent the skin from rubbing against footwear. Painful corns can be treated by regularly trimming the excess skin layers. Patients should avoid trimming corns by themselves, as this may exacerbate the pain and increase risk of infection. Most dorsal corns can be treated without surgery. When surgery is indicated surgical options for dorsal corns must address the underlying claw toe/hammer toe condition often via a PIP joint fusion.
Claw toes/Hammer toes – Painful toe tips (027)
In claw toes/hammer toes (Figure 1), the toes are abnormally bent at the middle and/or end joints (proximal and/or distal interphalangeal joints). When the toe deformity causes the tips of the toes to be pressed into the ground, activities such as walking can cause calluses to form at the toe tips. As a result, patients often experience pain at the tips of their toes. Painful toe tips can be treated by wearing comfortable loose-fitting shoes and adding padding such as a soft orthotic to footwear. Patients who present with the early stages of a claw toe/hammer toe deformity, when the toes are still flexible, are typically advised to wear hammer toe splints or other commercially available device (ex. Figure 2). These devices may help to keep the toes straighter and potentially prevent the toe tips from driving into the sole of the shoe. Surgical treatment for claw toe deformities that lead to painful toe tips will address the underlying claw toe/hammer toe condition.
Claw toes/Hammer toes- Unstable MTP Joint (029)
In addition to the middle and end joints of the toe, claw toe deformity also affects the metatarsophalangeal (MTP) joint (Figure 1). The MTP joint is located at the ball of the foot (base of the toes). Patients who have a claw toe deformity present with hyperextension of the MTP joint which makes the bone at the base of the toes (the metatarsal head) more prominent. This hyperextension can lead to pain in this area (metatarsalgia) and eventually an unstable MTP joint through two related mechanisms.
- The first mechanism involves the plantar plate, which is a ligament located at the base of the MTP joint. The plantar plate is responsible for keeping the MTP joint stable. When the MTP joint is repetitively loaded (ex. during walking) the joint may hyperextended with each step leading to wear and tear on the plantar plate. Eventually the plantar plate can tear or rupture. In patients with a claw toe deformity, an unstable MTP joint occurs when the plantar plate becomes damaged from years of MTP loading and hyperextension.
- The second mechanism through which a claw toe can cause MTP joint instability is inflammation of the entire joint lining (synovium). In patients with claw toes or hammer toes, bending of the toes at the middle joint (proximal interphalangeal joint) transfers weight to the MTP joint at the ball of the foot. Therefore, whenever a patient with a claw toe deformity walks, there is increased weight and loading on the MTP joint. This added pressure can lead to increased inflammation around the joint (MTP joint synovitis) eventually with resulting instability of the MTP joint.
Treatment
Non-Operative Treatment
Most claw toe deformities can be treated non-operatively. The literature describes a number of potential treatments including:
- Applying pads to the area involved. There are numerous commercially available devices, which can be highly effective in reducing the deformity and providing padding or off-loading the areas of prominence.
- Toe spacers and Hammer toe splints (Figure 2). Some commercially available products splint the toes in an improved position. These devices may only provide short-term correction of the toe deformity, but for many patients this can improve their symptoms when the walk and use shoes.
- The use of the wide and deep-toe box. A shoe with more room up front might be better able to accommodate the deformity and make a huge difference in the patient’s symptoms.
- A soft pre-fabricated orthotic to create cushioning over the toe region can be helpful, particularly if the symptoms occur at the tip of the toes.
- Trimming painful calluses. If prominent calluses have developed, trimming these back on a regular basis can be very helpful.
- Dynamic intrinsic muscle exercises. This has been proposed as a way to lessen the progression of claw toe deformity. Exercises, such as trying to pick up tissues with the toes, may be beneficial to keep the toes supple.

Operative Treatment
Surgery is occasionally recommended to correct claw toes that cannot be successfully treated non-operatively. There are a variety of surgical procedures that have been described to treat claw toes, and often a combination of procedures is performed. Because the claw toe deformity occurs as a result of a muscle imbalance, tendon transfer or lengthening may be needed in order to produce a succesful long-term surgical correction –and minimize the risk of a recurrence. Common procedures that may be used in combination with others include:
- Straightening the Toe (Proximal Interphalangeal (PIP) joint resection). If there is a fixed deformity at the PIP joint (the first “knuckle” of the toe), this joint can be removed, or repositioned in a straightened position and then fused with some type of fixation, often a wire insert through the toe. This joint may not fully heal with bone, but even a fibrous union (scar tissue) in a straight position will be effective.
- MTP joint (joint at the base of the toe) soft tissue release (capsulorraphy/capsulotomy). The MTP joint at the base of the toe flexes up, therefore the top part of the joint capsule (soft tissue) becomes very stiff and contracted over time. It is often necessary to release this contracted tissue, in order for the joint to fall back into its normal position. The MTP joint is held with a temporary wire in the new “straighter” position.
- Extensor tendon lengthening. Often the tendons that pull the toe upwards (long extensor tendons originating from the extensor digitorum longus muscle) will become contracted and tight. These tendons can be lengthened or simply released to allow the toes to fall back into an improved position. If released the little toe extensor may be anchored to the foot so the associated muscle, the extensor digitorum longus, can assist in dorsiflexion of the foot.
- Flexor to extensor tendon transfer [Girdlestone-Taylor procedure]. This procedure involves a release of one of the tendons that pulls the toe downwards (the flexor digitorum longus) at the tip of the toe (distally), and a transfer of this tendon to the top of the toe (dorsal aspect of the proximal phalanx). This procedure aims to convert one of the primary deforming forces leading to clawing of the toes into a force that helps correct the deformity. It produces a fairly predictable correction of the toes, however, the surgery is slightly more involved than some of the other procedures.
Recovery from Surgery
It is important to understand that the recovery from any toe surgery is often more prolonged than a patient expects. During the healing process, an increase in blood flow to the involved toe occurs. This creates swelling and pain in the toes. This swelling and discomfort can persist for many weeks, or even months. It is common to still have swelling and stiffness in the toes 4-6 months post-surgery. The patient should be prepared to limit their activity for a period that is often longer than they think, or would like.
Potential Complications
General Complications
The usual list of general post-surgical complications may occur with a claw toe correction. This includes the potential for:
- wound healing problems
- infection
- nonunion (if the PIP joint is fused)
- local nerve injury to the nerves that provide sensation to the tips of the toes
- Deep Vein Thrombosis (DVT) – very uncommon
- Pulmonary Embolism (PE) – very uncommon
Specific Complications
Complications that are specific to claw toe corrections include:
- Malunion: It not uncommon for the toe to heal in a position that may not be perfectly straight. Minor degrees of deformity will be mostly a cosmetic concern, which is why almost all surgeons discourage patients from having toe surgery if the concerns are mostly cosmetic. In severe cases, the toe may be notably crocked (significantly malpositioned), even to the point where further surgery is required.
- Recurrence of the Deformity: Another potential complication includes failure to fully correct the claw toe deformity, or the potential for recurrence of the deformity over time.
- Loss of blood supply to the tip of the toe: The blood supply to the tip of the toe can be tenuous. There are two small arteries (one on either side of the toe) which supply blood to the tip of the toe. It is not uncommon for one of these vessels to be absent. If the blood supply to the tip of the toe is lost the tissue will die and it may be necessary to amputate part, or all of the toe.
- Stiffness: It is not possible to straighten a claw toe and have the involved joints move normally. A good surgical outcome is a painless stiff, straight toe with the joints properly lined up.
Printable handout Complete Claw Toes Webpage
Edited by Stephen Pinney MD, on October 9th, 2025. Previously edited by Robert Leland, MD, and Michael Castro, DO