
Acquired Adult Flatfoot Deformity
(Progressive Collapsing Foot Deformity, Posterior Tibial Tendon Dysfunction)
Summary
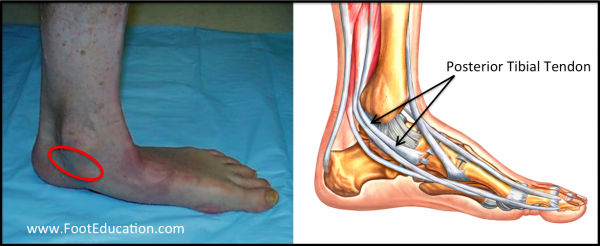
Acquired adult flatfoot deformity (AAFD) is a painful foot deformity associated with stretching out and dysfunction of the strong posterior tibial tendon on the inside of the ankle with a worsening flatfoot deformity. This condition was previously called chronic posterior tibial tendon insufficiency and is presently being renamed “progressive collapsing foot deformity“. Patients with acquired adult flatfoot deformity are typically middle aged individuals that report chronic pain on the inside of their foot and ankle. There is often a history of longstanding flatfeet (Figure 1) with this deformity now worsening and becoming quite painful. Symptoms of pain usually developed gradually as a result of overuse. However, symptoms may start with a specific often minor injury (the straw that breaks the camels back). Typically, the pain associated with acquired adult flatfoot deformity is localized on the inside (medial) aspect of the ankle (see circle in Fig. 1) along the course of the posterior tibial tendon. Pain on the outside of the ankle is also common due to compression loading through the bones on the outer aspect of the ankle (sinus tarsi impingement). Acquired adult flatfoot deformity commonly occurs in middle aged individuals who often have a history of flatfeet. Increased weight, an increase in activity level, and a stiffening (contracture) of the calf muscle may all serve to precipitate symptoms. This condition can often be treated without surgery by strengthening the involved muscles and tendons and bracing the ankle. When non-operative treatment fails, surgery can improve alignment and pain. However, while improved realignment and function of the foot can often be achieved the recovery time until maximal improvement is achieved is often greater than a year.
Listen to a Podcast on Painful Flatfeet
Summary Handout Acquired Adult Flatfoot Deformity
Watch Video: Acquired Adult Flatfoot Deformity
Background
Acquired adult flatfoot deformity is a condition that goes by many names including progressive collapsing foot deformity or posterior tibial tendon dysfunction. It may also be referred to as pes planus, a fallen arch, an abnormally pronated foot, or simply a painful flatfoot deformity. Acquired adult flatfoot deformity is a chronic foot condition where the soft-tissues (including the posterior tibial tendon, deltoid and spring ligaments) on the inside aspect of the foot and ankle are subject to repetitive load during walking and standing. Over time, these structures may stretch out or fail and become painful, swollen, or incompetent. A flat foot can be a normal variant and does not necessarily need treatment if it is non-painful and does not limit function. In other words, some people have “normal appearing arches,” some people have “high arches,” and other people have “pronated, or flat appearing arches.”
Clinical Presentation of Acquired Adult Flatfoot Deformity
Patients with acquired adult flatfoot deformity are often middled aged with a history of flatfeet. Foot pain usually develops gradually, but may occur suddenly if there is a precipitating, often minor, injury. Other risk factors for the development of symptoms include: being overweight, having a stiff calf muscle (ex. following an ankle injury), or a sudden increase in weight-bearing activities. All of these directly or indirectly lead to repetitive loading and attritional injury to the posterior tibial tendon and soft-tissues on the inside of the ankle. When these supporting structures fail, the result is pain, a limp, and often a change in the alignment of the foot. Acquired adult flatfoot deformity is typically associated with a worsening flatfoot deformity, leading to increased strain on the supporting structures on the inside of the ankle, and loading through the outer aspect of the ankle and foot. Typically patients describe pain and swelling on the inside (medial) of the ankle which can result in significant disability. However, some patients will also experience pain over the outside (lateral) aspect of the ankle and hind-foot, because of the resultant deformity and pressure or impingement on the lateral structures of the foot and ankle leading to sinus tarsi impingement. Patients may walk with a limp or, in advanced cases be markedly disabled due to pain.
Physical Examination
Looking at the patient when they stand will usually demonstrate a flatfoot deformity or a pronated foot (marked flattening of the medial longitudinal arch). The front part of the foot (forefoot) is often splayed out to the side, leading to the presence of a “too many toes” sign (Figure 2). This sign is present when the toes can be seen from directly behind the patient.

Posterior tibial tendon dysfunction may affect the patient’s walking, as the patient will have pain with weight-bearing and the dysfunctional posterior tibial tendon can no longer stabilize the arch of the foot when weight is placed on it. There is often tenderness to touch and swelling over the inside of the ankle just below the bony prominence (the medial malleolus). This area corresponds to the course of the posterior tibial tendon. With palpation there may also be pain in the outside aspect of the ankl. This pain originates from impingement or compression of two bones on the outside of the ankle.
A single-leg heel rise test is used to determine whether the posterior tibial tendon is intact or whether it has become dysfunctional. If the patient can stand on one foot and raise the heel off of the ground 3-5 times, then this suggests that the posterior tibial tendon is intact (Figure 3 [Left]). If they are unable to do this, the posterior tibial tendon is likely dysfunctional (Figure 3 [Right]).

Imaging Studies
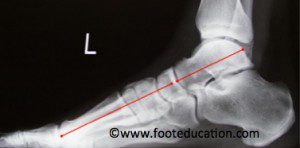
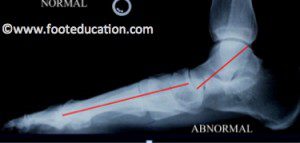
X-Rays of the foot taken while weight bearing allows the physician to assess the extent of the flatfoot deformity (Figures 4a and 4b).
MRI is usually not indicated for patients with acquired adult flatfoot deformity, as the diagnosis and the classification can be established on physical examination. However, if there are other clinical signs that suggest either a problem within the ankle, the subtalar joint, (intra-articular pathology) or another source of pain, then an MRI may be indicated. In some instances if surgery is being contemplated a weight-bearing CT scan may be indicated.
Classification
There are a number of classification systems for Acquired adult flatfoot deformity. One of the more widely accepted classification system divides the condition into four categories. Classifying the various stages of a condition can help guide treatment and prognosis. However, classifying conditions can be an inexact science and there is commonly disagreement between providers as to what “stage” condition a patient has (i.e poor interobserver reliability).
Stage 1 Acquired Adult Flatfoot Deformity (Posterior Tibial Tendon Dysfunction)
Patients with stage 1 posterior tibial tendon dysfunction have pain and swelling on the inside (medial) of the affected ankle. This area of pain and swelling corresponds to inflammation and irritation to the posterior tibial tendon. Patients often also have an underlying flatfoot deformity. However, the posterior tibial tendon is still functional so patients with a stage 1 deformity are still able to go up on their toes and perform a single leg heel rise, even though this motion may create pain.
Stage 2 Acquired Adult Flatfoot Deformity (Posterior Tibial Tendon Dysfunction)
Patients with stage 2 posterior tibial tendon dysfunction also have pain and swelling on the inside of the involved ankle as well as a noticeable flatfoot deformity (see above photos). However, in a stage 2 deformity the posterior tibial tendon is no longer working –either because it has become too stretched out, or it has ruptured. As a result, patients with a stage 2 deformity are unable to rise up on their toes. In fact, the inability to perform a single-leg heel rise is one of the defining features of a stage 2 acquired adult flatfoot deformity. Patients often walk with a limp as they are not able to push off on their toes normally. However, the flatfoot deformity is supple, meaning the foot is freely movable and a “normal” position can be restored by the examiner.
Stage 3 Acquired Adult Flatfoot Deformity (Posterior Tibial Tendon Dysfunction)
Patients with stage 3 posterior tibial tendon dysfunction have all of the symptoms and associated flatfoot deformity of patients with a stage 2 deformity except in addition their hindfoot joints are now stiff and have evidence of arthritis (some loss of cartilage). A prolonged flatfoot deformity causes uneven loading of the hindfoot joints (ex. the subtalar joint and talonavicular joint) which over time leads to stiffness and cartilage loss in these joints. This results in the inability to “correct the foot” to a normal position (loss of hindfoot joint motion). While a stage 3 deformity represents a flatfoot deformity that has become stiff because of hindfoot arthritis it is often difficult to tell when a stage 2 deformity actually becomes a stage 3 deformity. This is because the hindfoot stiffness and cartilage loss occurs on a spectrum. Expert orthopaedic foot and ankle surgeons may disagree over whether a patient has a stage 2 or a stage 3 deformity.
Stage 4 Acquired Adult Flatfoot Deformity (Posterior Tibial Tendon Dysfunction)
Patients with a stage 4 acquired adult flatfoot deformity have ankle arthritis or an ankle deformity as the defining feature. Like stage 3 deformities these patients have stiffness and/or arthritis in the joints below the ankle (subtalar and talonavicular joints). However, in addition, their ankle joint (tibiotalar joint) is also affected. With a long-standing flatfoot deformity, the ligaments on the inside of the ankle (deltoid ligaments) can become stretched out and the outside of the ankle joint takes a disproportionate load with weight-bearing. This eventually causes the deltoid ligament to excessively stretch out and/or the cartilage on the outside of the ankle joint to be worn away (ankle arthritis). If the deltoid ligament on the inside of the ankle becomes excessively stretched the ankle joint becomes unstable and will demonstrate a tilted appearance on X-ray. Whereas ankle arthritis occurs in a stage 4 deformity due to uneven loading on the outside (lateral) aspect of the ankle joint. Imagine a tire on a car that is put on at a crooked angle leading to uneven wear on one side of the tire. The same type of phenomena occurs in a stage 4 acquired adult flatfoot deformity leading to excessive loading with cartilage wear and arthritis on the lateral aspect of the ankle joint, and excessive traction on the inside of the ankle joint with subsequent stretching out of the deltoid ligament.
Treatment
Non-Operative Treatment
Nonoperative treatment of stage 1 and 2 acquired adult flatfoot deformity can be successful.
General components of the treatment include:
- The use of comfort shoes.
- The use of an over-the-counter (store-bought) or custom made orthotic insoles to support the arch
- Activity modification to avoid exacerbating activities and strengthening to build support.
- Weight loss if indicated.
Specific components of treatment that over time can lead to marked improvement in symptoms include:
- A high repetition, low resistance strengthening program (Alvarez Protocol)
- Appropriate ankle bracing or a medial longitudinal arch support.
If the posterior tibial tendon is intact, a series of exercises aimed at strengthening the elongated and dysfunctional tendon can be successful. In stage 1 or 2 deformities, this may be combined with an ankle brace and an off-the-shelf or custom made orthotic insert which may help to support the arch.
Operative Treatment
Operative treatment may be indicated for those patients that have stage 2 or higher dysfunction and have failed nonoperative management. The principles of operative treatment of stage 2 deformities include:
- Transferring another tendon to help serve the role of the dysfunctional posterior tibial tendon (usually the flexor digitorum or flexor hallucis longus is transferred)
- Restoring the shape and alignment of the foot. This moves the weight bearing axis back to the center of the ankle.
Changing the shape of the foot can be achieved by one or more of the following procedures:
- Cutting the heel bone and shifting it to the inside (Medializing calcaneal osteotomy)
- Lateral column lengthening restores the arch and overall alignment of the foot.
- Medial column stabilization, which stiffens the ray of the big toe to better support the arch.
- Lengthening of the Achilles tendon or Gastrocnemius. This will allow the ankle to move adequately once the alignment of the foot is corrected.
Stage 3 acquired adult flatfoot deformity may be treated operatively with a hindfoot fusion (arthrodesis). This is done with either a double or triple arthrodesis – fusion of two or three of the joints in hindfoot through which the deformity occurs. This is typically performed in such a way that the underlying foot deformity is corrected first.
Potential Surgical Complications
- Wound-healing problems
- Infection
- Failure to heal the bone (non-union) that has been cut or joints that have be fused
- Deep Vein Thrombosis (DVT), (blood clot forms in the leg)
- Pulmonary embolism, (blood clot travels to the lungs)
- Neurological injury
- Vascular Injury
- Continued pain and deformity
- Recurrence of deformity and pain
Recovery from Surgery
The recovery from surgery is dependent upon the particular combination of procedures that are performed. However, if cutting and repositioning bones or fusing joints is required, (as it usually is) a typical recovery would be:
- Healing Phase: 6-8 weeks of non-weightbearing is usually required
- Rehabilitation Phase: a period of gradual rehabilitation following the Healing Phase.
It is common for a patient to take 4-6 months to achieve much of their recovery, and 12-18 months before they reach their point of maximal improvement.
Printable Summary Handout of Acquired Adult Flatfoot
Printable handout -Copy of Full Webpage
Edited by Stephen Pinney MD. June 3rd 2026. Previously edited by: Steven Neufeld, MD